FHIR New Zealand Patient Summary IG
0.7.0 - ci-build
![]()
FHIR New Zealand Patient Summary IG
0.7.0 - ci-build
![]()
FHIR New Zealand Patient Summary IG, published by Health NZ | Te Whatu Ora. This guide is not an authorized publication; it is the continuous build for version 0.7.0 built by the FHIR (HL7® FHIR® Standard) CI Build. This version is based on the current content of https://github.com/tewhatuora/fhir-nzps/ and changes regularly. See the Directory of published versions
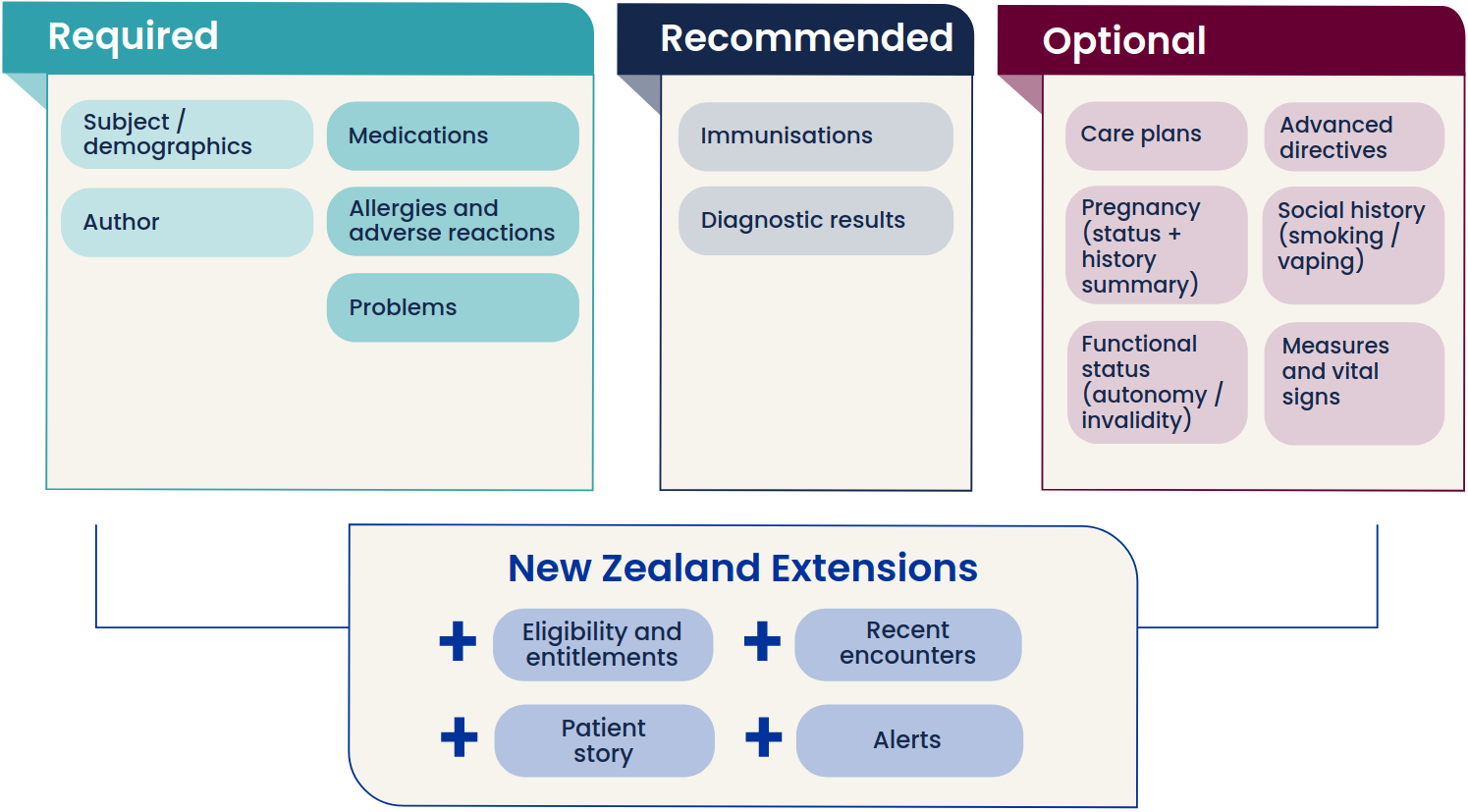
NZPS is an extensible data set specification that will build on the set of data blocks presented here. New requirements can be expected to emerge from IPS’s own further development, as well as from local initiatives. The initial scope of the NZPS covers the content areas shown in the data blocks below.
Figure 1: The NZPS initial contents
| Content area | What it contains | |
|---|---|---|
| Demographics | The person’s name, birth date and contact details, plus other identity, demographic, eligibility and enrolment information as recorded in the National Health Index (NHI) and National Enrolment System (NES) for everyone receiving public health services. The NHI number is the national health identifier and key to this information. | |
| Problems | Core personal health information centres on a concise statement of the problems and conditions affecting the person, including long term conditions and other current health issues. It includes pregnancy and can be an alert such as being immunocompromised. | |
| Medications | Core personal health information includes structured and coded data about each of the prescription medications in the person’s current or recent use. The data set includes prescription and dispensing details, including the indication for the medicine and the dosage. Over-the-counter medicines, traditional medicines, alternative medicines and supplements can be included. | |
| Allergies & Intolerance | Core personal health information includes a record of each known allergy or propensity for adverse reactions to some substance. All unresolved allergies and propensities are included. In each case, the medicine, food or other substance that is the causative agent is recorded, along with the manifestation of the allergy or adverse reaction, and its overall criticality. Some examples are a severe tongue swelling reaction to a certain medicine, an anaphylactic reaction to peanuts, a severe eye swelling reaction to cat allergen. | |
| Immunisations | Core personal health information includes a record of each of the person’s vaccinations. This should be a complete history or as much as known. The vaccine product, target disease and details of each vaccination event are recorded. The forthcoming Aotearoa Immunisation Register (AIR) will be the system of record for all vaccinations received in New Zealand or overseas. | |
| Diagnostic results | Test results relevant to the person’s health condition and risk, including pathology results, radiology results, medical imaging results, endoscopy reports, clinical results, consumer entered diagnostics and diagnostic results of all kinds. Some results are recorded in a time series. | |
| Smoking & vaping |
The core personal health data set includes the person’s smoking and vaping status. Health professionals follow an ABC pathway to ask, offer brief advice and provide cessation support to anyone smoking, and these interventions are recorded. | |
| Measurements & vital signs | The physiological measurements and vital signs that are important to the person’s life stage, health risks and conditions are recorded in the core personal health data set. These measurements include height, weight, heart rate, respiratory rate, blood pressure, body temperature, head circumference and body surface area, to name a few. | |
| Care plans | A care plan in the context of a patient summary is a simple record of each consultation, test, treatment or other activity planned in managing some health condition or towards some health goal. For example, a care plan may exist to communicate a forward view of the planned care for a person with COVID. The same person may have other care plans for other conditions. Appointments, orders, referrals and discharge summaries are common sources of care plan data. | |
| Functional status | An individual’s ability to perform normal daily activities required to meet basic needs, fulfil usual roles and maintain health and well-being | |
| Advance directives | Provision for healthcare decisions in the event that, in the future, a person is unable to make those decisions. Contains structured information related to the identity and address details of the decision maker and a description of all known patient's advance directives; this may reference a legal document. As there may be multiple directives it may be that the content is organized as a list. Furthermore, there may just be a reference to a document (sometimes known as a Living Will) rather than simple text. This reference may be an URL but is not restricted to just that form of reference. | |
| Encounters | Core personal health information includes a record of the person’s recent encounters and interactions with health providers and the health system. This includes planned and unplanned encounters, in-person and online, at home or at a facility. Common types of encounter includes visits and online consultations with a GP, allied health professional or specialist. |