
Central Cancer Registry Reporting Content IG
2.0.0-ballot - STU 2 Ballot
![]()
Central Cancer Registry Reporting Content IG
2.0.0-ballot - STU 2 Ballot
![]()
Central Cancer Registry Reporting Content IG, published by HL7 International / Public Health. This guide is not an authorized publication; it is the continuous build for version 2.0.0-ballot built by the FHIR (HL7® FHIR® Standard) CI Build. This version is based on the current content of https://github.com/HL7/fhir-central-cancer-registry-reporting-ig/ and changes regularly. See the Directory of published versions
| Page standards status: Informative |
Population-based cancer surveillance is critical in North America for cancer control activities aimed at reducing the morbidity and mortality of cancer, the second leading cause of death in the United States (U.S.). Population-based public health central cancer registries across the U.S. are mandated to collect complete and timely cancer diagnostic, treatment, and outcome data from hospitals, physician offices, treatment centers, clinics, laboratories, and other sources. Recent shifts in cancer treatment from hospital settings towards ambulatory healthcare settings are increasing the importance of ambulatory (non-hospital) healthcare providers (e.g., non-hospital, non-laboratory health care practitioner, physician or dental office, ambulatory surgery center, cancer treatment center, etc.) authorized/required to report a cancer case to the public health central cancer registry for cancer surveillance.
Regional, state and territorial public health central cancer registries collect, manage, and analyze data about cancer cases and cancer deaths. Cancer surveillance is a complex system that captures longitudinal data from multiple data sources using a variety of methods. In addition to recording the occurrence of each reportable cancer (or tumor), the reporters provide information to public health central cancer registries on the diagnosis, treatment and vital status. Reporting requirements may vary by hospital, state, district, territory, or province. Please note for the purposes of this implementation guide the term, “reportable cancer” is inclusive of all tumors reportable to a public health central cancer registry. The North American Association of Central Cancer Registries (NAACCR) Standards for Cancer Registries, Data Standards and Data Dictionary, describes the standards of tumor reportability for national standard-setting organizations in North America.
Public health central cancer registry data are used for surveillance, development of comprehensive cancer control programs, and healthcare planning and interventions. Improved accuracy and completeness of cancer surveillance data impacts all areas of public health interventions. Data also provides baseline and performance measures for cancer-related interventions designed to reduce cancer incidence or improve early detection. Identification of disparities among various population subgroups in stage at diagnosis or in treatment received can inform interventions to reduce these disparities and reduce the cancer morbidity and mortality in minority or disadvantaged populations.
The National Program of Cancer Registries (NPCR), established in 1992 by the U.S. Congress with enactment of the Cancer Registries Amendment Act (Public Law 202-515), is funded and managed by the Centers for Disease Control and Prevention’s (CDC) Cancer Surveillance Branch (CSB) in the Division of Cancer Prevention and Control (DCPC). The Surveillance Epidemiology and End Results (SEER) Program of the National Cancer Institute (NCI), initiated by the National Cancer Act of 1971 (PL 92-218), began collecting population-based cancer incidence data in 1973. Together, NPCR and SEER programs collect data for the entire U.S. population and produce the annual United States Cancer Statistics (USCS). CDC and NCI monitor the burden of cancer, including disparities among various population subgroups and provide data for research, evaluation of cancer control activities, and planning for future healthcare needs at both the state and national levels. Complete and high-quality cancer reporting traditionally relies primarily on data from acute care hospitals and, more recently, pathology laboratories.
Advances in medicine and changes in the healthcare delivery system now allow patients to obtain their care outside the acute care hospital setting. Data collection systems from ambulatory healthcare providers such as physician offices and radiation therapy centers are not as standardized or complete with respect to reporting of cancer occurrences and treatment. When reporting does occur, it may be through a manual process of identifying reportable cases and submitting paper copies of the medical record, or the central registry may send certified tumor registrars (CTRs) to ambulatory healthcare provider offices to abstract the information manually or electronically from the paper-based medical records. The Health Level 7 (HL7) Clinical Document Architecture (CDA®) Release 2 Implementation Guide (IG): Reporting to Public Health Cancer Registries from Ambulatory Healthcare Providers, Release 1, DSTU Release 1.1 – US Realm is the first standard for ambulatory care to use when electronically transmitting cancer cases to the central cancer registry. The CDA IG is part of the Office of the National Coordinator (ONC) Meaningful Use and identifies the content and structure for reporting from physician electronic health records (EHRs) to central cancer registries (CCRs), but it does not use HL7 Fast Healthcare Interoperability Resources (FHIR®). These processes are very resource intensive, time-consuming, prone to errors in transcription, and inherently less secure. This leads to under-reporting of certain types of cancers, especially those now diagnosed and treated primarily outside of hospitals, such as in dermatology, urology, and hematology, as well as under-reporting of treatment information across most types of cancer.
Standards specifications provided in this document are designed to facilitate the implementation of an automated electronic process for the identification and reporting of cancer cases, treatment, and outcomes using ambulatory healthcare provider EHR systems to create a cancer event report and submit it to public health central cancer registries. Automated electronic reporting is expected to reduce labor (for the ambulatory healthcare providers and public health central cancer registries), and increase the security, completeness, timeliness and accuracy of cancer surveillance data.
Cancer reporting from all healthcare providers (e.g., hospital, laboratory and ambulatory) for public health surveillance is mandated at the state and territory level. Legislation requiring cancer reporting by healthcare providers exists in all states with some variation in specific requirements. United States federal law Public Health Service Act (42 USC 280e-280e-4; Public Law 102-515), as amended, authorizing the National Program of Cancer Registries, specifies that each federally-funded registry must have a legislative "means for the statewide cancer registry to access all records of physicians and surgeons, hospitals, outpatient clinics, nursing homes, and all other facilities…”. The National Cancer Act of 1971 (Public Law 92-218) gives the Director of NCI the authority to “collect, analyze, and disseminate all data useful in the prevention, diagnosis and treatment of cancer.”
The Health Insurance Portability and Accountability Act (HIPAA, or the Act), P.L. 104-191, enacted on August 21, 1996, includes provisions related to insurance coverage and a section that is relevant to electronic reporting of healthcare information. The regulation implementing the HIPAA privacy provisions allows public health exemptions for disclosure without patient consent of individually identifiable health information. A discussion of HIPAA as it relates to reporting to Cancer Registries outlines details relating to HIPAA and cancer reporting.
The section identifies the need and specific details of central cancer registry reporting.
Cancer is a mandatory reportable disease; every state has public health law/regulation requiring information to be reported to a central cancer registry about all cancers diagnosed or treated within that state. Central cancer registries are population-based cancer registries that collect data on all cancer diagnosed in residents in a defined geographic area. The main sources of information include information from treatment facilities (e.g., hospitals, clinics/physician offices), diagnostic services (e.g., pathology laboratories) and vital statistics (e.g., death certificates). Central cancer registries have an emphasis on epidemiology and public health to determine patterns among various populations, monitor cancer trends over time, guide planning and evaluation of cancer control efforts, help prioritize health resource allocations and to advance clinical, epidemiologic and health services research 1.
Although cancer reporting for public health surveillance is mandatory, certain types of cancers, treatments, and biomarkers are currently underreported to central cancer registries. This underreporting is because more patients are being diagnosed or treated outside of a hospital setting, such as in ambulatory clinical practices (dermatology, gastroenterology, urology, hematology, etc.). Due to lack of interoperability, these disparate systems are challenged with reporting complete and timely data in a standardized format to cancer registries, and subsequently manual processes are necessary to obtain and process often incomplete data to meet surveillance reporting requirements. Even with reporting requirements, cancer surveillance is complex given the heterogeneous nature of the disease, numerous diagnostic and prognostic factors, and multiple medical encounters that produce data from a variety of non-harmonized data sources.
Challenges include:
These challenges make it difficult for registries to synthesize information in a timely and actionable way. Automation of cancer case registry reporting will reduce the burden of manual or other non-standardized data collection processes that currently exist.
The goal of the Central Cancer Registry Reporting Content IG is to automate the capture of cancer cases and cancer treatment information and provide incidence data faster for research and public health. The Central Cancer Registry Reporting Content IG will leverage existing FHIR® infrastructure to transmit cancer case information primarily from ambulatory care practices to central cancer registries. Additionally, this use case aims to identify data standards that allow for the collection and transmission of these data electronically from EHRs automatically rather than relying on labor-intensive manual processes and duplications of effort.
In-Scope
Out-of-Scope
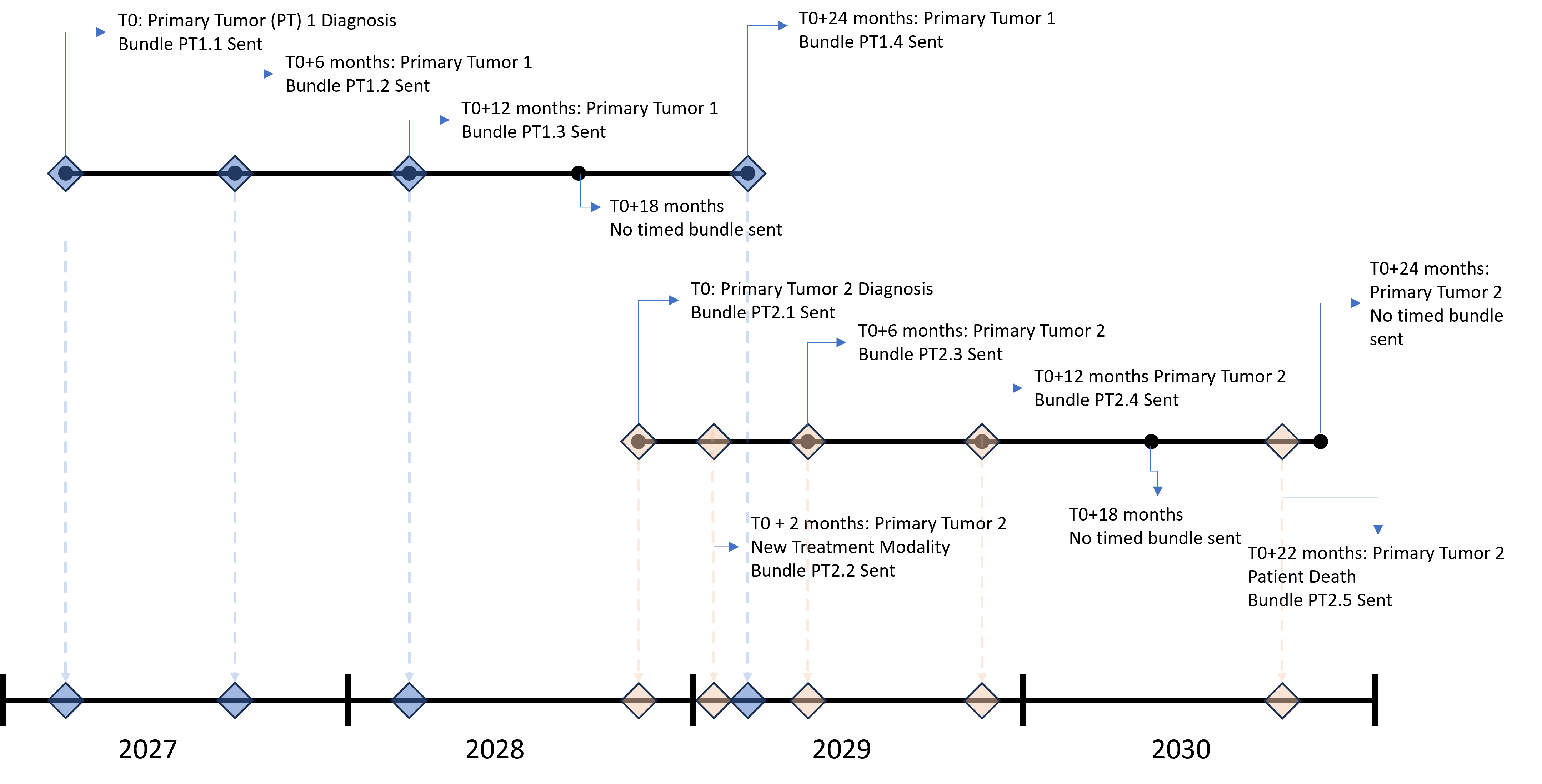
To limit the number of reports sent to registries, this IG contains specific reporting intervals and criteria for both encounter-based and content-based triggering of when a report is sent to a Central Cancer Registry (CCR).
For the initial report (T0), when a qualifying encounter occurs, the patient record will be queried at 15 days post-encounter and (if necessary) 30 days post encounter for the presence of the following content:
If all content is present at the 15 day check, then an initial encounter-based report will be sent to the registry. If any of the content is missing, the initial report will be sent at T0+30 days regardless of content status.
The intent of this report is to initiate an incidence case.
After the T0 bundle is sent, incremental reports containing patient information and new information will be sent based on availability of specific content. The following additions to the patient record will trigger an incremental report:
After 12 consecutive months of no trigger criteria or upon patient death, reporting will stop.
NOTE: Central Cancer Registry Reporting is tumor-based, not patient-based. Every tumor will have its own triggering and reporting timeline.
The following describes a realistic history of a patient’s journey from discovering a breast lump of concern through diagnosis, treatment, monitoring, and follow-up for breast cancer. This scenario describes a journey where all the patient’s providers starting with her visit to the oncologist are in a single cancer center and using a single Electronic Health Record (EHR). The diagnostic testing information and biopsy results are provided for context, but in this scenario are conducted by providers outside of the cancer center. This information will be reported to the cancer registry through other means outside of this scenario. When information in the scenario does not map on to Central Cancer Registry Reporting Content (CCRR) IG profiles, we provide examples using US Core or mCode FHIR IG, as indicated in the CCRR IG detailed specification. We also condense some repeated patterns. For example, we only show one example of MedicationAdministration, when in reality there are several different medications included in the patient’s chemotherapy regimen.
Patient History
Demographics: Patient Amy Shaw is a 38 year old multiracial Latina female.
Occupation & Industry: Amy has been a factory worker for an oil-based paint and floor finish manufacturer for 15 years.
Health History: No significant family history of breast cancer. She leads an active lifestyle, with no smoking or excessive alcohol use. She has insulin-dependent diabetes, first diagnosed when she was a child.
Initial Symptoms: In January 2023, Amy notices a lump in her left breast.
Diagnosis
Primary Care Visit: On 3/5/2023, she visits her general practitioner (GP) after noticing that the lump has persisted. The doctor conducts a physical exam and orders a mammogram with ultrasound as needed.
Diagnostic Testing: Mammogram and ultrasound performed on 3/10/2023 confirm a suspicious mass in the area of concern. GP recommends a biopsy. A week later (3/17/2023), Amy presents to the radiology office for a core-needle breast biopsy. The specimen from the needle biopsy is sent to the pathology laboratory for analysis and interpretation.
Biopsy Results: Pathology confirms triple-negative infiltrating duct carcinoma of the left breast. The laboratory sends the pathology report to the state cancer registry, the radiologist, and the primary care provider.
PCP Visit: She is referred by her PCP to an oncologist for treatment. PCP sends the pathology report to the oncologist.
Oncologist Consultation: Amy has a consultation with an oncologist, Dr. Joseph Nichols, on 3/21/2023 (extension:assertedDate in Central Cancer Registry Reporting Primary Cancer Condition Profile). This visit establishes T0 for purposes of determining triggers for reporting to the central cancer registry. Dr. Nichols orders a CT and MRI. He documents her cancer diagnosis of infiltrating duct carcinoma (extension:histologyMorphologyBehavior) of the left (extension:lateralityQualifier) breast (bodySite) in her medical record, and notes Histologic test (procedure) as the diagnostic confirmation method (extension:cancer-status-evidence-type).
CT and MRI are performed on 3/24/2023 and Dr. Nichols receives the results on 3/29/23. Results confirm that the cancer is 4cm, localized, with no adenopathy or visible metastases. After reviewing the results, on 4/4/23 Dr. Nichols documents the clinical stage classification as cT2, cN0, cM0, and Stage Group IIA, AJCC 8th Edition.
4/5/23: The diagnosis of cancer associated with the encounter triggers an initial report to be generated and sent to the central cancer registry. (T0+15 days: Encounter-based (EB) bundle EB.1)
Treatment and Monitoring
Chemotherapy: On 4/10/2023 Amy begins chemotherapy to shrink the tumor before surgery.
4/10/23: The administration of cancer-related medications is a non-encounter-based (NEB) trigger for an incremental report to be generated and sent to the central cancer registry. (NEB.1)
Surgical Intervention: On 11/8/23 she undergoes a lumpectomy followed by sentinel lymph node dissection.
11/8/23: The surgical procedure triggers an encounter-based incremental report to be generated and sent to the central cancer registry (EB.2)
Radiation Therapy: On 1/31/24 Amy begins external beam radiation treatment (mcode-radiotherapy-course-summary.mcode-radiotherapy-modality-and-technique.mcode-radiotherapy-modality.value) to eliminate any remaining cancer cells. She receives this treatment for 8 weeks, with her last visit on 3/31/24.
3/31/24: The completion of radiation therapy triggers a non-encounter-based incremental report to be generated and sent to the central cancer registry. (NEB.2)
Monitoring and Follow-Up: Amy undergoes frequent follow-ups to monitor for recurrence, blood tests, physical exams every 3-6 months for the first 3 years, and annual mammograms. Monthly checks for new information that meet the trigger requirements could result in additional reports generated and sent. These are not included in this journey.
Figure 2.1 below illustrates a sample central cancer registry reporting timeline for the Patient Journey described above.
This section outlines the high-level interactions between the various actors and systems listed above.
Figure 2.2 below depicts the interactions between actors and systems when the Data Submitter is part of the Data Source Organization.
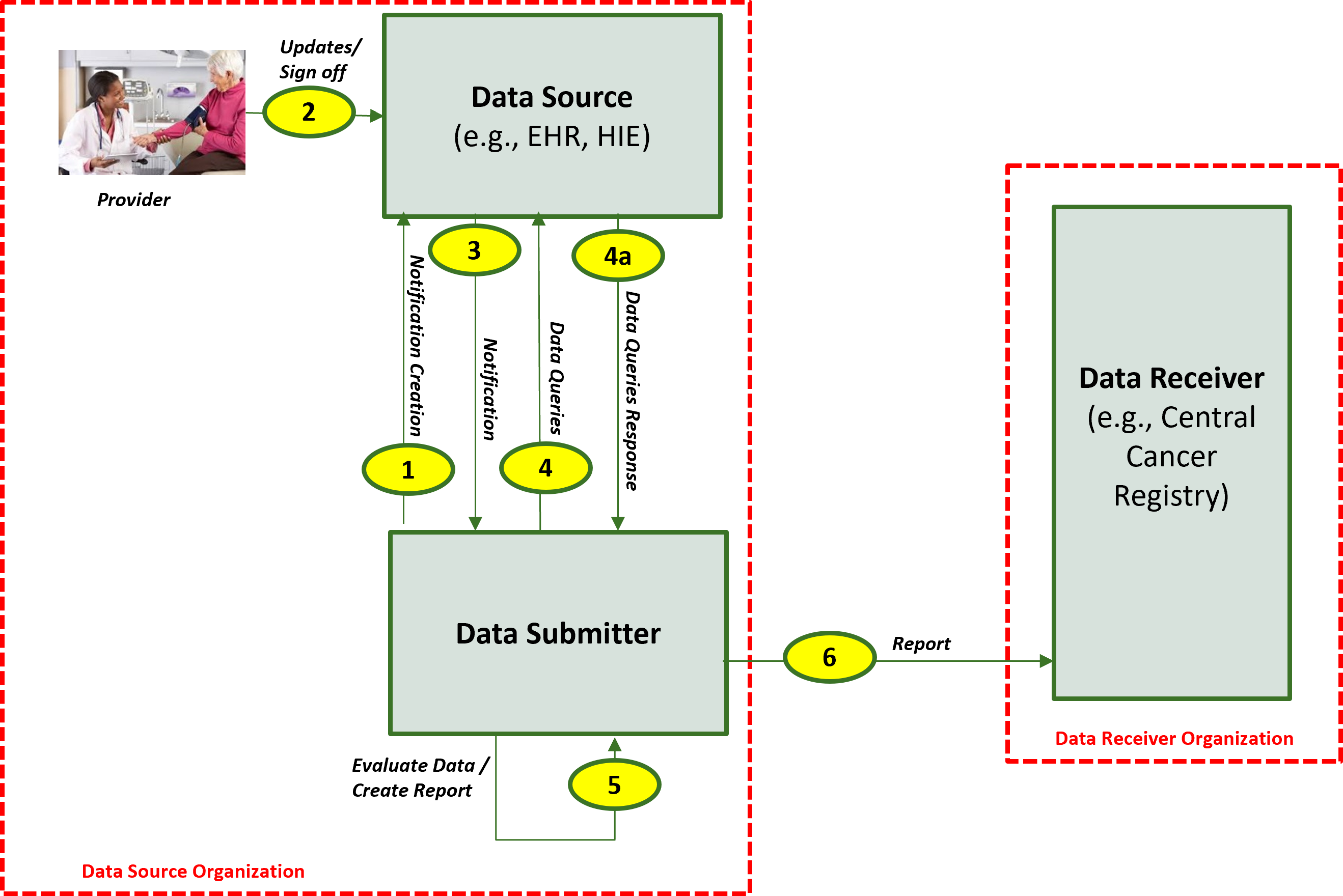
The descriptions for each step in the above diagram include:
Figure 2.3 below depicts the interactions between actors and systems when the Data Submitter is integrated with the Data Source.
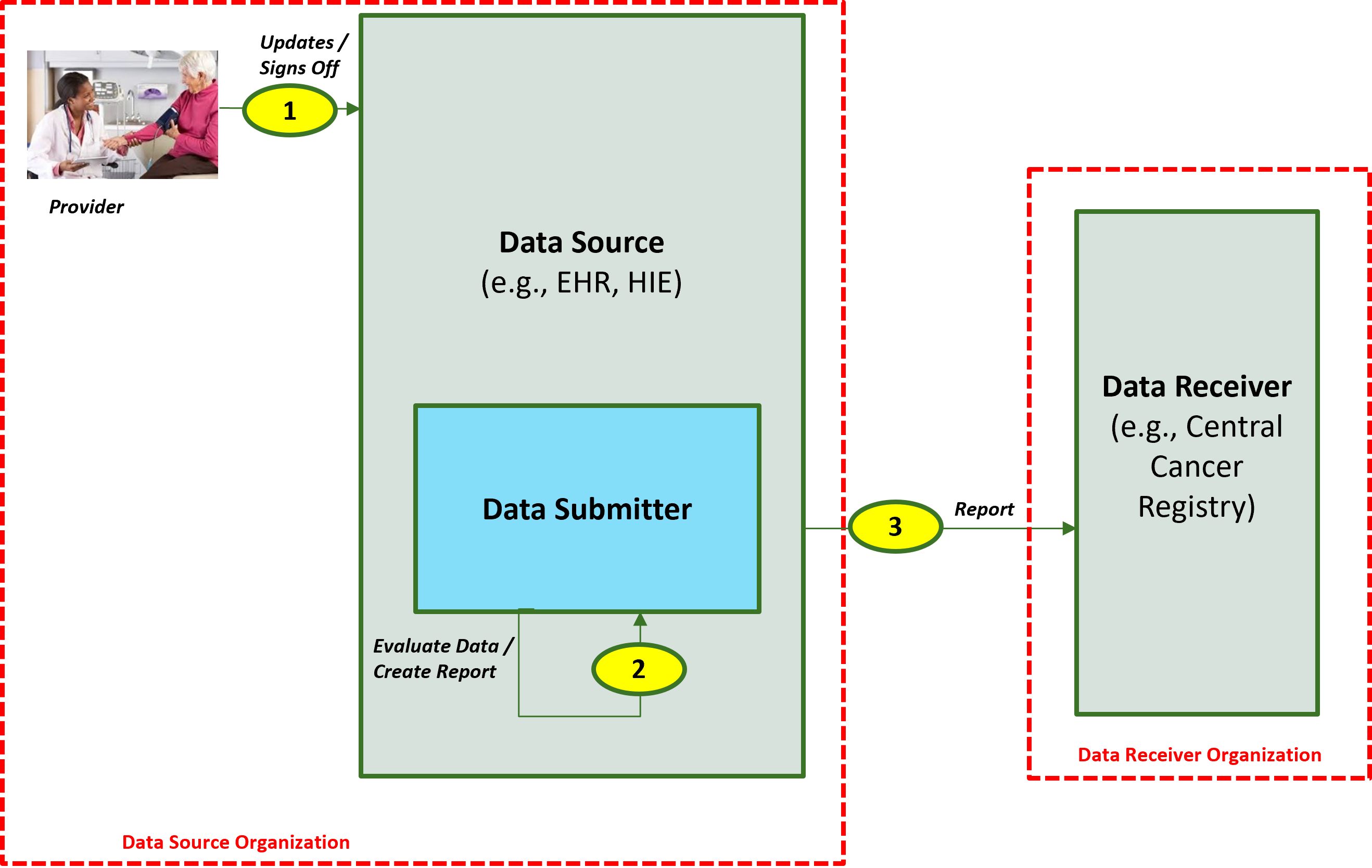
The descriptions for each step in the above diagram include:
The CDC Central Cancer Registry Program has identified the list of conditions against which the patient's data is evaluated for reporting purposes. If a patient has any of the conditions listed in any of the value sets identified below, the patient's data qualifies for reporting to the central cancer registry. These are not explicitly included in the IG as they will be maintained externally.
| ValueSet Name | ValueSet OID/CodeSystem OID | ValueSet URL |
| Cancer [Benign or Borderline CNS Tumors] (Disorders) (ICD10CM) | 2.16.840.1.113762.1.4.1146.1403 / 2.16.840.1.113883.6.90 | https://vsac.nlm.nih.gov/valueset/expansions?pr=all&rel=Latest&q=2.16.840.1.113762.1.4.1146.1403 |
| Cancer [Malignant Neoplasms] (Disorders) (ICD10CM) | 2.16.840.1.113762.1.4.1146.1402 / 2.16.840.1.113883.6.90 | https://vsac.nlm.nih.gov/valueset/expansions?pr=all&rel=Latest&q=2.16.840.1.113762.1.4.1146.1402 |
| Cancer [Unspecified Skin Cancer, Benign Carcinoid Tumor, in situ Cervical Cancer, Intraepithelial Neoplasia, History Cancer, Complication of Cancer or Treatment] (Disorders) (SNOMED) | 2.16.840.1.113762.1.4.1146.1405 / 2.16.840.1.113883.6.96 | https://vsac.nlm.nih.gov/valueset/expansions?pr=all&rel=Latest&q=2.16.840.1.113762.1.4.1146.1405 |
| Cancer [Benign or Borderline CNS Tumors] (Disorders) (SNOMED) | 2.16.840.1.113762.1.4.1146.1406 / 2.16.840.1.113883.6.96 | https://vsac.nlm.nih.gov/valueset/expansions?pr=all&rel=Latest&q=2.16.840.1.113762.1.4.1146.1406 |
| Cancer [Unspecified Skin Cancer, Benign Carcinoid Tumor, in situ Cervical Cancer, Intraepithelial Neoplasia, History Cancer, Complication of Cancer or Treatment] (Disorders) (ICD10CM) | 2.16.840.1.113762.1.4.1146.1404 / 2.16.840.1.113883.6.90 | https://vsac.nlm.nih.gov/valueset/expansions?pr=all&rel=Latest&q=2.16.840.1.113762.1.4.1146.1404 |
| Cancer [Malignant Neoplasms] (Disorders) (SNOMED) | 2.16.840.1.113762.1.4.1146.1407 / 2.16.840.1.113883.6.96 | https://vsac.nlm.nih.gov/valueset/expansions?pr=all&rel=Latest&q=2.16.840.1.113762.1.4.1146.1407 |
1 Menck, H., Gress, D. and Griffin, A., 2011. Cancer Registry Management Principles and Practices for Hospitals and Central Registries. 3rd ed. Dubuque, IA: Kendall Hunt. ISBN: 978-0-7575-6900-5.
IG © 2021+ HL7 International / Public Health. Package hl7.fhir.us.central-cancer-registry-reporting#2.0.0-ballot based on FHIR 4.0.1. Generated 2025-12-15
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change