
Da Vinci Risk Adjustment Implementation Guide
3.0.0-ballot - STU 3 Ballot
![]()
Da Vinci Risk Adjustment Implementation Guide
3.0.0-ballot - STU 3 Ballot
![]()
Da Vinci Risk Adjustment Implementation Guide, published by HL7 International / Clinical Quality Information. This guide is not an authorized publication; it is the continuous build for version 3.0.0-ballot built by the FHIR (HL7® FHIR® Standard) CI Build. This version is based on the current content of https://github.com/HL7/davinci-ra/ and changes regularly. See the Directory of published versions
| Page standards status: Trial-use |
The Da Vinci Project member organizations have identified the need of standardizing how risk adjustment coding gaps are communicated between payers and providers. This implementation guide (IG) specifies standardized risk adjustment coding gap reports and provides guidance to query the coding gap reports from a Payer for one or more patients. Standardizing the reporting structure helps lessen the burden on the providers in processing the reports so they can more easily address the patients’ care needs. This standardized structure also supports the Payer sharing information that they have but the providers may not, such as data from other providers’ claims, lab results, filled prescriptions, etc.
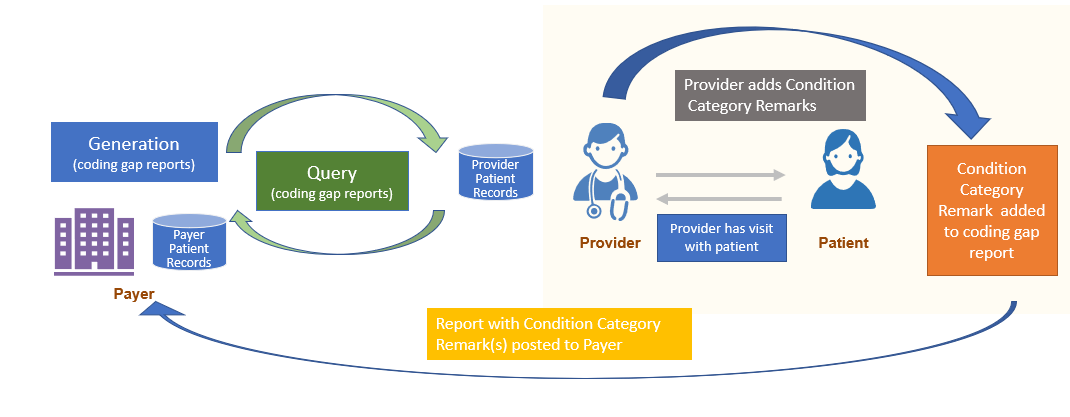
This IG also provides mechanisms enabling the feedback loop from Provider to Payer. Providers may add a Condition Category Remark(s) to the Risk Adjustment Coding Gap Report to indicate that they took some action(s) for a specific coding gap on the report and communicates that back to the Payer. However, if the Provider identifies a coding gap that is on the report needs to be closed or invalidated based on medical record review, this feedback process is done using the Risk Adjustment Data Exchange MeasureReport, which allows the Provider to send the supporting clinical evaluation evidence to the Payer. This feedback loop is important for achieving the goal of improving the accuracy and completeness of risk adjustment.
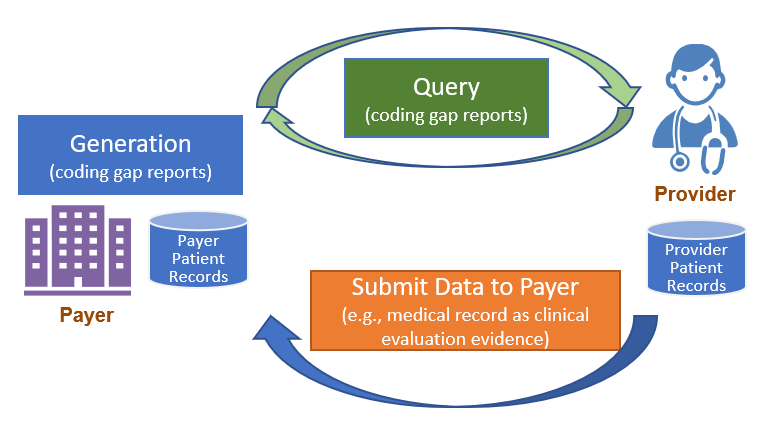
Figure 2.1-1 shows a high level overview of the risk adjustment workflow, which consists of three main phases: Report Generation, Report Query, and Submit Data to Payer. Detailed guidance for each phase is provided on a separate page under the Methodology section.
For a complete introduction and background to Report Generation, please visit Report Generation Introduction and Background. Report generation describes two different approaches to generate a Risk Adjustment Coding Gap Report, which are referred to as Assisted and Generated in this IG.
You will find more details on the two approaches at Report Generation Approaches.
The Client can query the Risk Adjustment Coding Gap Report once they are generated. For example, the Payer acting as the Reporting Client can query reports based on search parameters and POST them to the Provider server. See the Report Query page for details and guidance.
Once the queried Risk Adjustment Coding Gap MeasureReports have been sent to the intended recipient, it can be filtered as defined by the EMR and their configuration options to ensure that only germane coding gaps (e.g., HCC gaps) are made available to providers. The Provider (or a software program acting on behalf of the Provider) determines whether the coding gap is currently valid, and whether the requested encounter data evidence exists to close the gap.
At that time, if the Provider wants to note the action they took regarding a Risk Adjustment coding gap, they can add that comment to the Risk Adjustment Coding Gap Report using the Condition Category Remark extension and return it to the Payer. This process is called Condition Category Remark.
Note: The Condition Category Remark extension is not intended to change the status of a Condition Category gap. To change the coding gap status, follow the Submit Data to Payer section of this guidance. Note that both a Condition Category remark and Submit Data to Payer can be generated at the time the Provider sees the patient if that is appropriate.
To return clinical data, the Provider will use the Risk Adjustment Data Exchange MeasureReport and FHIR Resful API to submit data to Payer. The Payer will then be able to use the provided patient data to update the data in their system that will be included on their next coding gap report generation.
See the Submit Data to Payer page for more details and guidance.
This section describes how a provider and payer can use the $risk-gap operation to support proactive clinical gap closure during a patient’s upcoming visit.
In this example use case, patient A is establishing care with a new primary care physician (PCP). Patient A has a scheduled appointment approximately one month from today. The clinic and payer exchange information related to potential risk conditions before and during the visit, enabling accurate and timely assessment.
contextId that’s provided in the HTTP header of the operation, as part of the pre-visit workflow for the upcoming encounter.
The payer responds with current risk gaps and suspected conditions, returning the same unique event identifier for linkage by using the Context Id extension of the Risk Adjustment Coding Gap Report profile. contextId) sent in the first $risk-gap API call since it is related to the same event/visit. Current/updated risk gaps, conditions, and corresponding information are returned in the API response, allowing the care team to address pending items during the encounter. Insurance eligibility is also verified as part of the preparation. contextId) for the event. Payer can utilize the unique identifier for the event to track/tie together when a request was received, date of the event, when PCP took an action on the condition.
By maintaining a consistent unique event identifier across pre-visit, encounter-time, and feedback transactions, this information can be used to monitor providers adoption rate, timing of assessing the condition, and determining incentive payments.
The overarching goal is to encourage providers to assess the condition when they are seeing the patient, versus waiting until the last couple months of the year. This real-time exchange supports higher accuracy in risk adjustment, more complete clinical documentation, and improved care coordination.
Member attribution establishes associations between providers and payers. The process of establishing and exchanging patient lists for risk adjustment coding gap reports is not in the scope of this implementation guide. One possible way of exchanging Member Attribution Lists between providers and payers is described in the Da Vinci - Member Attribution (ATR) List implementation guide.
Different entities can play different Roles in different scenarios. The Actors in this implementation guide are Payer and Provider. Their roles as Client and Server are described below.
Client:
Server:
The Methodology section of this implementation guide describes these Actors in more detail in the context of report generation, report query, and data submission steps of risk adjustment lifecycle and adding of Condition Category remarks to the Risk Adjustment Coding Gap report.
IG © 2021+ HL7 International / Clinical Quality Information.
Package hl7.fhir.us.davinci-ra#3.0.0-ballot based on FHIR 4.0.1.
Generated
2026-04-05
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change