ACT-NOW Implementation Guide
0.4.0 - ci-build
![]()
ACT-NOW Implementation Guide
0.4.0 - ci-build
![]()
ACT-NOW Implementation Guide, published by Te aho o te kahu - Cancer Control Agency. This guide is not an authorized publication; it is the continuous build for version 0.4.0 built by the FHIR (HL7® FHIR® Standard) CI Build. This version is based on the current content of https://github.com/davidhay25/actnow/ and changes regularly. See the Directory of published versions
This page describes the resource graph developed to represent the ACT-NOW data standard as FHIR resources.
The general flow by which a patient receives cancer treatment, and the corresponding FHIR representation, is as follows.
A patient has a diagnosis of cancer, as determined on histological and clinical grounds. This diagnosis is represented as a Condition resource, with Observation resources representing the histological and other findings that led to that diagnosis. In particular there are a number of 'ancillary' tests that are performed for particular diagnoses - such as Estrogen receptor status of Breast cancer. These tests are represented as Observations, and are important in determining the treatment protocol.
Once diagnosed, a treatment plan is determined. Each cancer type has a number of possible treatment regimens that can be applied, each of which consists of a number of cycles of treatment - specifically administration of medications. The treatment regimens are represented as PlanDefinition and ActivityDefinitions, and there is a separate IG that defines how this is done.
The Clinician/s planning the treatment will select the regimen to apply, and this is represented for the individual patient in a CarePlan resource. Currently, the mechanics of this is outside of the scope of this guide, but the CarePlan resource is used to support any future expansion of the scope.
A regimen of treatment consists of a number of separate cycles of medication administration which may be repeated a number of times. Both regimen and cycle are represented as CarePlan resources, with the Cycle plan being related to the Regimen plan using the 'partOf' reference. The CarePlan.category value indicates whether the plan is a regimen or a cycle (or, indeed, something else).
When a regimen is started, there are a number of initial measurements taken (such as Body Surface are). These are represented as Observation resources referenced from the plan using 'supportingInfo' references. When the regimen completes (or is cancelled) there are other Observations made that record the outcome of treatment, and possible the reason for cancellation. These Observations have a reference back to the plan using the Observation.basedOn reference.
Similarly, when a cycle starts and ends there are Observations which may be recorded.
An individual medication administration is related to the Cycle plan under which it was given. If the medication was actually given to the patient it is represented as a MedicationAdministration resource. If it is a prescription given to a patient it will be represented as a MedicationRequest resource.
The following diagram shows an example of a small set of data for a patient, with only a single cycle. Note that all the resources will have a reference to the Patient, and some to a Practitioner - these are not shown for clarity.
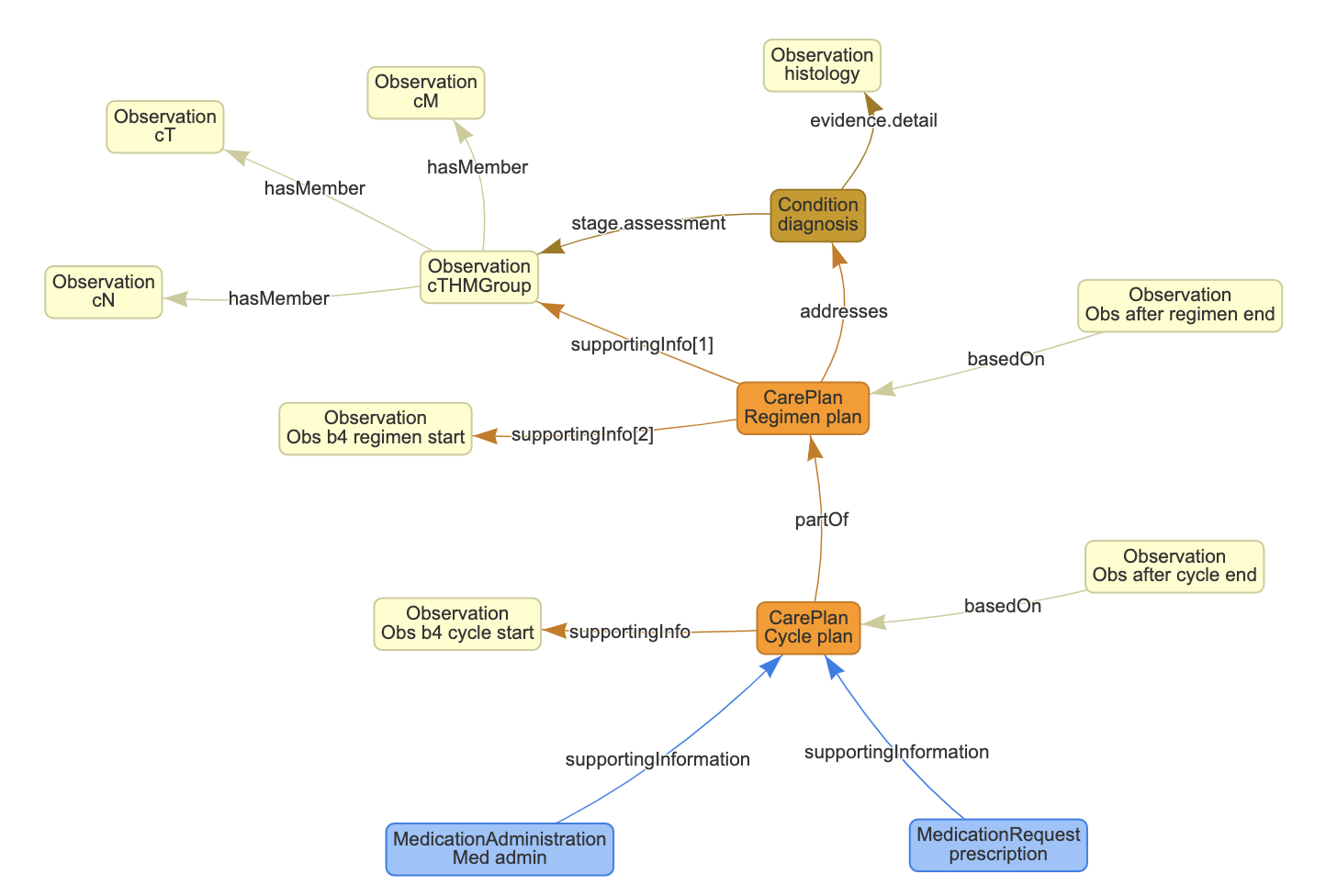
The image is shown with a central column of the Diagnosis (with supporting histology and assessment), then the regimen and cycle care plans. Usually there will be multiple cycle plans for any given regimen.
To the left are Observations made before the start of a regimen / cycle - blood tests and other ancillary studies. These have a reference from the CarePlan to the resource using a 'supportingInfo' reference as (in theory) the observations would exist prior to the CarePlan being created.
To the right are Observations made when the regimen / cycle ends, mostly blood tests. The reference is from the Observation to the CarePlan (using a 'basedOn' reference) as they are created after the CarePlan. The profiles that define these measurements include:
(These might also be taken prior to the regimen starting, in which case the reference is 'addintionalInfo' from CarePlan to Observation)
Outcome measures are recorded as extensions on the CarePlan itself, as the CarePlan has to be updated anyway to update the status, and it makes it easier to read that information. These can be seen on the Regimen CarePlan profile and the Cycle CarePlan profile
At the bottom are the medication administrations (ie medications actually given to the patient like an IV infusion) and prescriptions (represented as a MedicationRequest).
Note that other resources and references between resources are certainly possible if appropriate, but the ones defined in this page are the base ones defined.
Most of the resources are created and not subsequently updated (other than any error correction). However, the CarePlans (regimen and Cycle) may be updated over time as their status. If the information were being submitted in real-time:
This all means that the CarePlans may have multiple versions, though only the most recent one is generally retrieved when querying the server (The history operations can be used to retrieve previous versions, though these are not considered in this guide).
All treatment follows a pre-determined regimen (pattern) of treatment (though can be adapted to the patient depending on their response to treatment). The regimens are defined in a separate IG (using a combination of PlanDefinition & ActivityDefinition resources ).
When a regimen is applied to a patient, it is represented as an instance of a CarePlan. It is possible for there to be a reference to the PlanDefinition using the instantiatesCanonical element, but this is not currently defined in this guide, as the instrastructure is not yet generally available.
There are a number of extensions defined which can be applied to the CarePlan - such as the intent of treatment or whether this treatment is part of a clinical trial.
The diagnosis is recorded as a Condition resource. If there is histology supporting the diagnosis, then that is represented as an Observation, and the Condition has an evidence reference to the Observation.
The CarePlan that represents the regimen being followed should have an addressses reference to the Condition
This records how advanced a tumour is, and is generally recorded using the 'TNM' mechanism which measures the Tumour size, Involvement of Local nodes and metastases.
Following the pattern of mcode these are recorded as 4 distinct Observations - One for each of the TNM measures, and a single 'summary' observation. The summary Observation has hasMember references to the individual Observations, and the regimen CarePlan has a supportingInfo reference to the summary Observation.
It is also possible for there to be a reference from the Condition to the summary Observation using the stage.assessment reference.
Commonly there are measurements made before treatment commences - for example Creatinine Clearance test to determine drug dosages or the ECOG score so that the effectiveness of treatment can be determined.
Generally these are recorded as Observations, and the regimen CarePlan will have a supportingInfo reference to them.
There are also measures that are made after the treatment ends - perhaps to record the effectiveness of treatment, or any damage caused by the medications. These are recorded as Observations, with a basedOn reference back to the regimen CarePlan
Each cycle of treatment is represented by a separate CarePlan resource - ie each cycle has its own CarePlan. The status of the CarePlan will be active when treatment defined by the cycle is being given and completed once the cycle has been completed.
If the cycle needs to be stopped early for any reason - such as patient intolerance - then the status will be revoked and there will often be an Observation that records the reason why. The Observation will have a basedOn reference back to the cycle carePlan.
Like the regimen CarePlan it is also possible to have measures made before and after the cycle commences and starts. These are recorded using Observations in the same way as for the regimen.
Sometimes a regimen needs to be cancelled before it is completed. For example the side effects of treatment are so severe as to warrant a new regimen being considered.
The regimen CarePlan status will be revoked and there will often be an Observation that records the reason why. The Observation will have a basedOn reference back to the regimen carePlan.
If this happens during a cycle of treatment, then the cycle CarePlan will also be updated as described above.
All medication administrations (actual delivery of the medication orally or parenterally) are recorded as MedicationAdministration resources.
The MedicationAdministration needs a reference back to the cycle CarePlan. This is done using a supportingInformation reference.
(As an aside, in FHIR release 5 there is a specific basedOn reference that might be used).
Sometimes measures are taken before or after medication administration. These are represented as Observations, and should have a reference to the cycle CarePlan via the basedOn reference.
The MedicationAdministration resource might also reference them using the spportingInformation reference.
If the patient was given a prescription for a medication - rather than having it administered by someone, then the apprppriate resource type is MedicationRequest. It also references the cycle CarePlan by a supportingInformation reference.