

Dental Data Exchange
2.0.0-ballot - CI Build
![]()
Dental Data Exchange
2.0.0-ballot - CI Build
![]()
Dental Data Exchange, published by Payer/Provider Information Exchange Work Group. This guide is not an authorized publication; it is the continuous build for version 2.0.0-ballot built by the FHIR (HL7® FHIR® Standard) CI Build. This version is based on the current content of https://github.com/HL7/dental-data-exchange/ and changes regularly. See the Directory of published versions
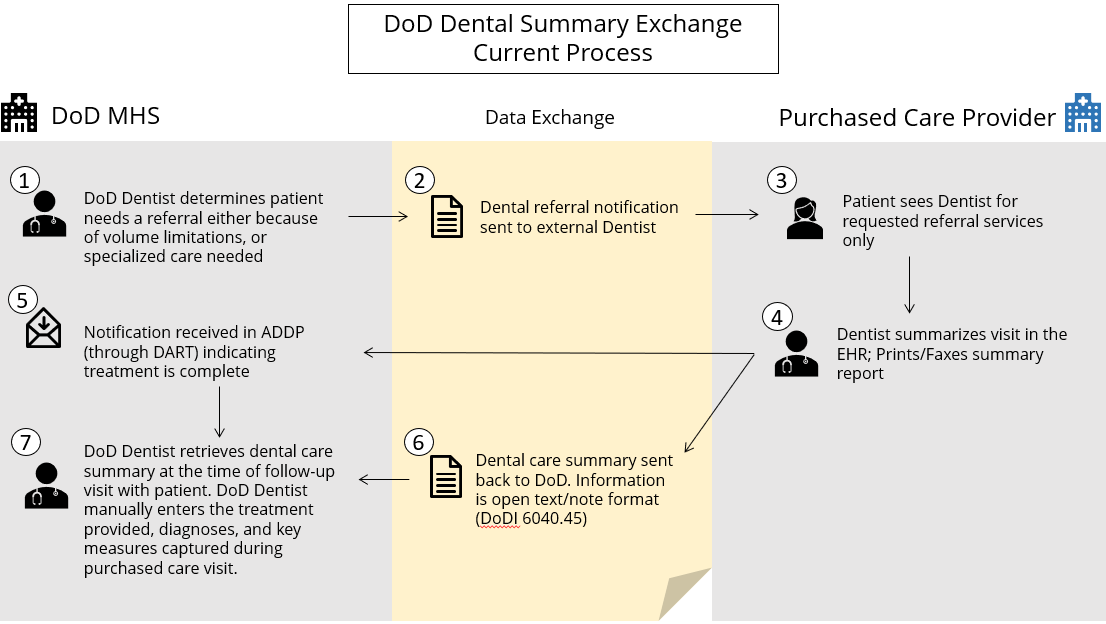
The project described the current workflow for sending and receiving medical to dental and dental to dental information to identify pain points and crucial gaps in the current state. The figure below represents a dental referral request from the Military Health System (MHS) of the US Department of Defense (DoD).
Figure 1: Dental Referral Request from the Military Health System
 |
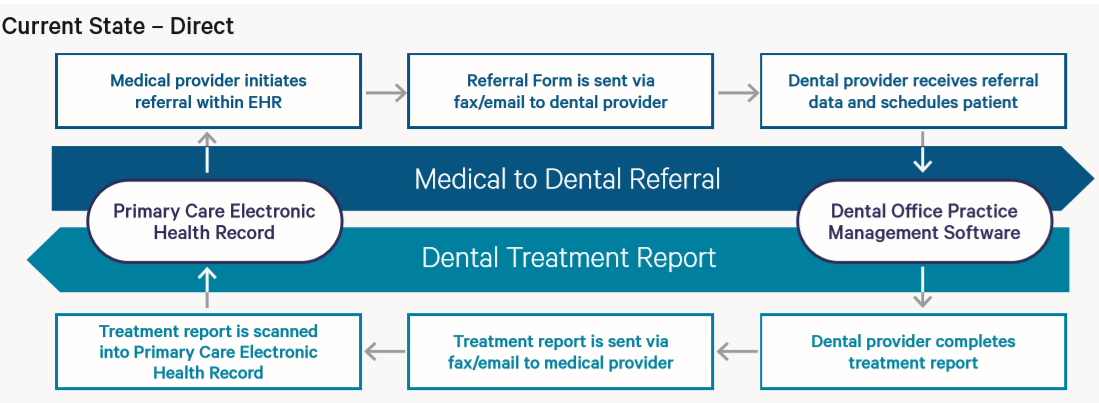
Currently, providers in the CareQuest Institute system initiate paper referrals (see MORE CARE Medical Provider Referral for Dental Care) which are shared with a dental provider via fax or e-mail who schedules the patient. The dental provider then treats the patient and returns a treatment report (See MORE CARE Dental Referral Treatment Report) to the medical provider via fax or email. This report is scanned into the patient’s primary care record. In this current workflow, the medical/dental is not electronically exchanged nor integrated electronically into the medical electronic health record (EHR) or dental health record.
Figure 2: Current State Workflow via FAX or Email
 |
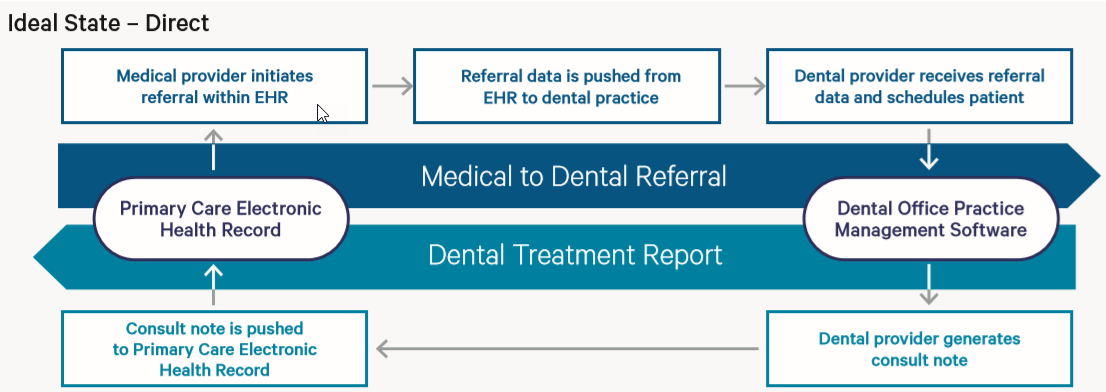
The ideal future state involves sharing the patient’s medical information via a referral electronically to the dental EHR to eliminate email and fax exchange, and reduce administrative time spent on referral management. Where possible, the data that is shared is electronically integrated into the dental EHR and the resulting treatment report is electronically sent back to the referring primary care provider (PCP).
Figure 3: Ideal State Workflow via Electronic Referral
 |
It is anticipated that these standards will have applicability and relevance outside of the specific use cases. For example, they may be used to standardize the transmission of data to plans and payers to develop utilization and quality metrics to enhance value-based care and payment methodologies. In addition, the standardization of the data elements embedded in the exchange will allow for more complete analysis of the connection between oral health and overall health.
IG © 2020+ Payer/Provider Information Exchange Work Group. Package hl7.fhir.us.dental-data-exchange#2.0.0-ballot based on FHIR 4.0.1. Generated 2025-04-07
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change