
Clinical Practice Guidelines
2.0.0 - STU2
![]()
Clinical Practice Guidelines
2.0.0 - STU2
![]()
Clinical Practice Guidelines, published by HL7 International / Clinical Decision Support. This guide is not an authorized publication; it is the continuous build for version 2.0.0 built by the FHIR (HL7® FHIR® Standard) CI Build. This version is based on the current content of https://github.com/HL7/cqf-recommendations/ and changes regularly. See the Directory of published versions
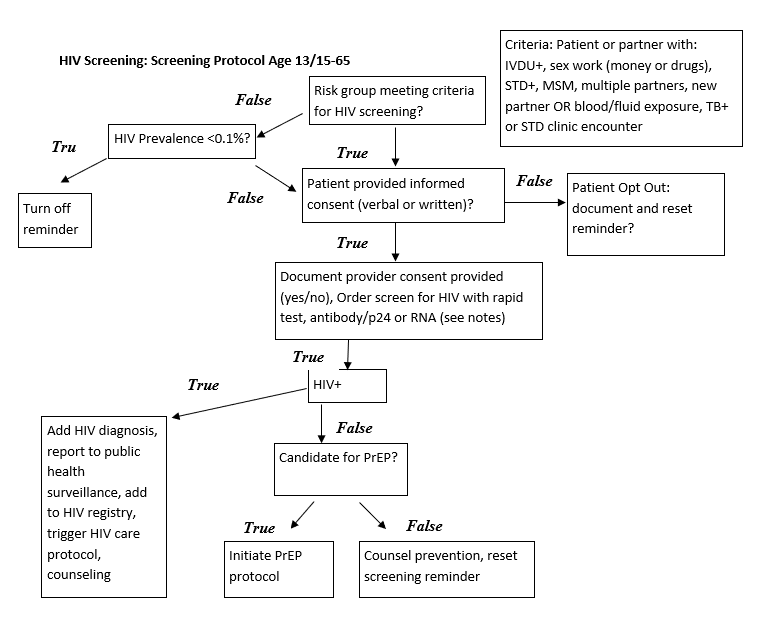
Recommends screening all individuals 13-65, including all pregnant women presenting from initial diagnosis through those presenting in labor. Recommends more frequent screening for individuals at high risk.
Supplemental Content USPTF June 2019 HIV Screening Screening for HIV Infection - US Preventive Services Task Force Recommendation Statement
Recommends screening all individuals 15-65, including all pregnant women presenting from initial diagnosis through those presenting in labor. Recommends screening for younger or older individuals who are determined to be at high risk. Recommends more frequent screening for individuals at high risk.
Screening for HIV Infection in Pregnant Women
Pregnant women in labor, recommend Rapid HIV test—otherwise routine HIV testing
HIV-1 RNA
IG © 2023+ HL7 International / Clinical Decision Support. Package hl7.fhir.uv.cpg#2.0.0 based on FHIR 4.0.1. Generated 2024-11-26
Links: Table of Contents |
QA Report
| Version History |
 |
Propose a change
|
Propose a change